Micropipetting is one of the first practical skills a life science student or new lab technician learns, and on the surface it looks straightforward. You select a volume, attach a tip, draw up a sample, and dispense it. In practice, though, it's a technique that takes time to get right, and small errors in posture, angle, or aspiration speed translate directly into inaccurate results. Teaching it well, and doing so at scale, is more difficult than most people outside the lab appreciate.
VR pipetting simulators give learners a way to repeat the technique as many times as they need, with instant feedback at each step, before they ever pick up a real pipette. This post looks at why that matters, what the evidence says, and what a simulator like PipetteSim™ covers in practice.
Why micropipette technique is harder to teach than it looks
A well-executed pipetting step involves more variables than the motion itself suggests. Volume selection, tip attachment, pre-wetting, aspiration angle, plunger depression speed, the position of the tip against the vessel wall, and the way you release the plunger: each of these affects the accuracy of the volume delivered. Get several of them slightly wrong at once and the error compounds.
Research into pipetting performance consistently identifies the user as the largest source of error in the lab, more so than the equipment itself. Poor or inconsistent technique translates directly into poor and inconsistent results; an experiment that should be reproducible isn't, because two scientists performing the same protocol are delivering slightly different volumes at each step. In environments where precision matters, such as ELISA assays, cell culture protocols, or any work involving scarce samples, that inconsistency has consequences.
The difficulty for trainers is that technique is largely kinaesthetic. You can watch a demonstration and follow written instructions, but the physical feel of the plunger, the angle of the arm, the speed of aspiration: these things are learned through doing, and they take repetition to become habit. A single supervised session is rarely enough.
What poor technique costs
The cost of pipetting errors shows up in a few different places. The most immediate is reagent waste: inaccurate volumes mean samples are consumed without producing usable data, and experiments have to be repeated. In labs working with expensive reagents or limited biological material, this adds up quickly.
There are also the downstream costs of rework. When results are inconsistent and can't be confirmed, the experiment has to run again. That takes time, consumes more reagents, and ties up equipment and personnel. In a biotech or CRO setting, repeated rework delays timelines and increases the cost of every project it affects.
Estimates from the calibration industry put the cost of a single pipetting error at between $400 and $1,000 when you account for data analysis, reagent waste, and additional payroll. Across a lab of ten technicians making two errors each per year, the annual cost can reach $20,000. Over five years, that exposure runs to $100,000. (Source: Transcat Pipettes)
Beyond direct costs, there's the harder-to-quantify issue of reproducibility. Life science research depends on results that can be replicated. If pipetting technique varies between scientists on the same team, the data they produce will vary too, and that variation undermines the reliability of everything built on top of it.
Where traditional training runs into limits
The standard approach to pipetting training involves a demonstration, followed by supervised practice with real reagents. This works reasonably well for small groups with a patient supervisor and enough time. It runs into difficulties at scale.
The first issue is resource consumption. Every practice repetition uses tips, consumables, and, depending on the protocol being practised, actual reagents. For universities teaching cohorts of undergraduate students, or CROs onboarding multiple new scientists at the same time, the cost of letting each person practice enough to build real confidence is not trivial.
The second issue is access. Lab time is scheduled, equipment is shared, and the supervisor who would normally provide feedback has other things to do. In practice, many learners get one demonstration and a limited opportunity to practise before they're expected to work independently. That's not enough repetition for technique to become reliable.
The third issue is consistency of feedback. In a supervised session, the quality and detail of feedback depends on the supervisor. Different trainers emphasise different things. If you're trying to standardise technique across a team, you need the feedback itself to be standardised, and that's difficult to achieve with manual instruction alone.
What VR practice adds
A VR micropipette simulator addresses the repetition problem. Because no physical reagents are consumed, the cost of each practice session is essentially zero once the equipment is in place. A learner can work through a protocol ten times, make the same mistake repeatedly, receive consistent feedback at the point the mistake happens, and correct it before the session ends. That kind of deliberate, failure-safe repetition is difficult to provide in a real lab environment.
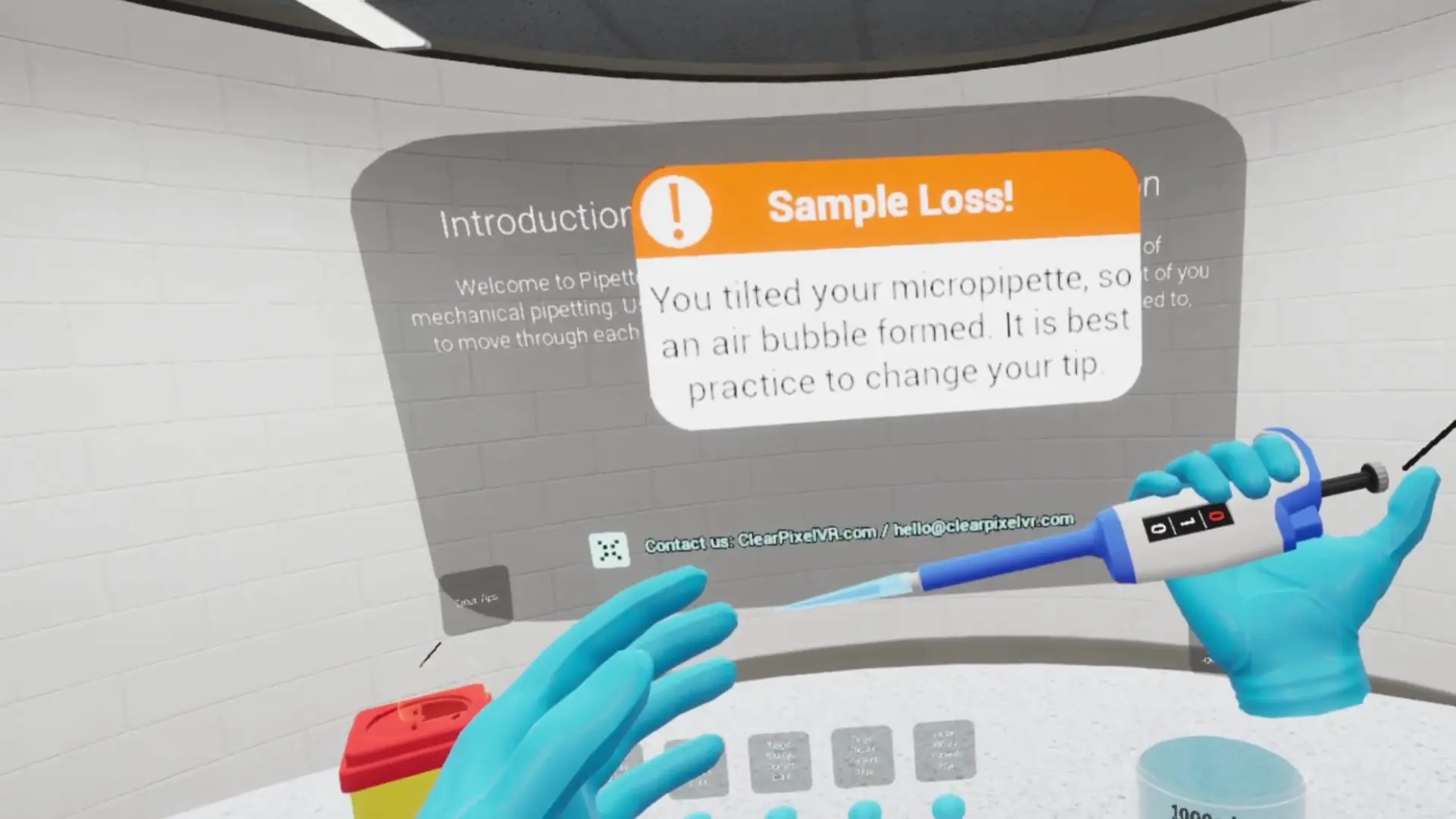
The feedback is also immediate and consistent. Rather than waiting for a supervisor to notice an error in technique, the simulator flags it as it occurs, whether it's the angle of aspiration, an incorrect volume setting, or a skipped step in the protocol. Every learner receives the same feedback, in the same way, every time.
What the research shows
A study by Petersen, Klingenberg, and Makransky at the University of Copenhagen looked specifically at whether performance in a VR pipetting simulation predicts real-world pipetting performance. Their finding was that it does: learners who performed well in the virtual environment also performed better on a real-life transfer test. The study also found that VR increased self-efficacy in all participants, meaning students came out of the virtual session more confident in their own ability, regardless of which group they were in.
The researchers were careful to note that VR performed best as a complement to real-world instruction rather than a replacement for it. Students taught entirely by a real-life instructor still made fewer errors on the transfer test than those taught only through VR. The practical conclusion is that VR is most valuable in the preparation and reinforcement stages, giving learners a way to build familiarity and repetition before supervised practice with real equipment, and to revisit the technique independently afterwards.
What PipetteSim™ covers
PipetteSim™ is clear_pixel's VR micropipette training platform, built specifically for life science education and lab training. It runs on a standalone Meta Quest headset, so there's no PC or lab setup required. It can be used in a teaching room, a library, or anywhere else with enough space to stand and move comfortably.
The simulator covers the mechanics of micropipetting in detail. Aspiration, dispensing, tip attachment, and tip ejection are all simulated with realistic interaction, and the platform includes multiple pipette models across common volume ranges (P20, P200, P1000) as well as multichannel options. Guided training modules walk learners through each stage with scored checkpoints, so there's a clear record of where errors occurred and what the learner's accuracy looked like across a session.
The repeat-practice model is central to how it works. A learner can run through a protocol as many times as they need, with the feedback system flagging errors at the moment they happen. The goal is to get technique right in the simulator, so that when the learner picks up a real pipette for the first time, the physical movement already feels familiar.
PipetteSim™ is already in use at Ewha Womans University, where it was integrated into the life sciences curriculum across a full semester. For more on that deployment and what the faculty observed, see our Ewha case study.
Who it works well for
There are three settings where VR pipetting practice tends to make the most difference.
- University life science departments. First-year students often arrive with no practical lab experience and need to build technique from scratch before they can participate meaningfully in supervised sessions. VR gives them a low-stakes environment to do that, without consuming lab resources or taking up supervisor time.
- CROs and biotechs onboarding new scientists. When multiple people join at the same time, or when onboarding happens continuously throughout the year, providing enough supervised pipetting practice for everyone to reach a consistent standard is hard to manage. VR practice standardises the baseline and reduces the load on experienced team members who would otherwise be running the same induction session repeatedly.
- Lab managers trying to standardise technique across a team. If technique varies between scientists, results will vary too. A shared VR training module gives everyone the same reference point for what good technique looks like, with the same feedback criteria applied consistently across the team.
In each case, VR practice works best when it's built into a broader training programme rather than used in isolation. The research supports a blended approach: VR for preparation and repetition, supervised practice for the hands-on transfer, and a real pipette in hand for the work that follows.
Related Reading
Sources
- Petersen, Klingenberg, Makransky (2022): Pipetting in Virtual Reality Can Predict Real-Life Pipetting Performance
- Transcat Pipettes: The Remarkable Cost of Pipette Errors
- Advanced Instruments: Pipettes as Sources of Error
- PipetteSim™ by clear_pixel VR
- Chung et al. (2025): Student performance in a hybrid laboratory model, PMC
Let's talk
Ready to see PipetteSim™ in action?
We'll walk you through the platform and discuss how it fits your training programme.
Contact us